

Background: Graft versus host disease (GVHD) is a life-threatening complication following allogeneic stem cell transplantation (AlloSCT), which results from allo-reactive donor T-cells reacting against human leukocyte antigen (HLA) disparate host antigens. Despite the use of prophylactic immunosuppresants, 40 to 70 percent of patients undergoing HLA matched related and unrelated transplants will develop grade II-IV acute GVHD (Goker et al, Ex Hem, 2001; Nademanee, Blood, 1995; Rutuu et al, BMT, 1997).CD34+ enrichment of GCSF mobilized peripheral blood stem cells (PBSCs) obtained by apheresis is a method for T-cell depletion to reduce the risk of Grade II-IV aGVHD but unfortunately maybe concomitantly associated with delayed immune reconstitution, increased opportunistic infection and/or malignant relapse. To circumvent these latter complications, we previously demonstrated the results of a CD34+ enrichment with mononuclear cell (MNC) addback fixed at 2x105 CD3/kg of recipient weight in pediatric MUD recipients demonstrating rapid engraftment, robust immune reconstitution, and a low incidence of Grade II-IV aGVHD (Geyer/Cairo, BJH, 2012).More recently, we demonstrated a similar approach in children, adolescents, and young adults with high-risk SCD following familial haploidentical stem cell transplantation resulting in a rapid engraftment, probability of 6.7% of Grade II-IV aGVHD and 90% 1-year OS (Cairo et al, JAMA Peds, 2020). This approach of PBMNC addback with a fixed dose of 2x105 CD3/kg facilitated the infusion of additional NK, NKT, B, DC, DC2 cells at that same time (Chu/Cairo et al, ASH, 2020).
Objective: To determine the safety, hematopoietic engraftment, probability of Grade II-IV GVHD following HLA related and unrelated PBSC transplantation following CD34+ enrichment with MNC cell addback (2x105 T-cell/kg fixed dose) in patients with malignant and non-malignant diseases.
Design/Methods: Eligible patients were enrolled on study. Patients received individualized conditioning regimens determined by the PI stratified by disease, disease status, and donor source and received CD34+ enriched products processed by using the CliniMACSâ CD34+ Reagent System (Miltenyi Biotec, Bergisch Gladbach, Germany). The CD34+ cell product was either infused or cryopreserved and stored until time of transplantation. A target of 5x106 CD34+/kg recipient weight with a PBMNC fixed dose of 2x105 T cell CD3 dose/kg was infused as we previously demonstrated (Cairo et al, JAMA Peds, 2020). Patients were followed for safety, engraftment, donor chimerism, probability of Grade II-IV aGVHD and chronic GVHD.
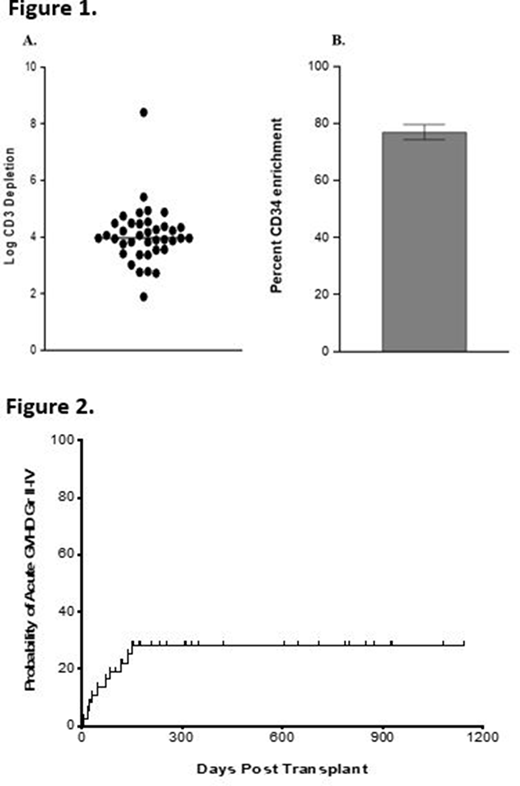
Results: Thirty-eight patients underwent HSCT with median age of 35.2 years (21 months to 71 years). Patients' disease status was as follows: complete remission (CR) 3 in 1 AML patient, CR2 in 8 AML patients, CR1 in 14 AML patients, CR2 in 4 ALL patients, CR1 in 2 ALL patients, PR in 1 MDS patient, Lymphohistiocytosis (n=1), Macrophage Activating Syndrome (n=1), Diamond Blackfan (n=1), Aplastic Anemia (n=2), Sickle Cell Disease (n=1), 1 CNL patient, CR2 in 1 Non-Hodgkins Lymphoma patient. Sixteen patients received allogeneic 10/10 HLA-matched unrelated donors, 5 from 9/10 HLA-matched unrelated donors, 12 from 6/6 HLA-matched sibling donors, 5 from related haplo donors. PB-HPC products contained 2x105 CD3/kg (±0.25 x 105), and 9.72x106 CD34/kg (±0.97 x106). After CD34 enrichment, the PB-HPC product processed was 76.09% CD34+ (±2.7%) (Fig. 1A) enriched with mean ± SEM log T cell depletion of 4.01 (±0.17) (Fig. 1B). The target HSCT dose per patient was 5x106 CD34/kg. Thirty-seven patients had myeloid engraftment and 32 patients had platelet engraftment with a median of 11 and 17 days, respectively. Six patients died prior to platelet engraftment - three due to multi-organ system failure following septic shock, two due to refractory disease, and one due to adenoviremia. Early and late peripheral blood chimerism was ³ 95% at 14- and 100-days following transplantation. The probability of grade II-IV aGVHD was 28.1% (CI95: 9.3-50.7) (Fig. 2). The probability of cGVHD was 4% (CI95: 0-63.5).
Conclusion: This study demonstrates safety, rapid hematopoietic engraftment, sustained donor chimerism of CD34+ enriched PBSC products with MNC cell addback with a fixed 2x105 CD3/kg dose in alloSCT recipients with a low probability of Grade II-IV aGVHD.and cGVHD.
Seiter:Novartis: Honoraria, Research Funding, Speakers Bureau; Celgene: Honoraria, Research Funding, Speakers Bureau; Incyte: Honoraria, Speakers Bureau; Sanofi: Honoraria, Speakers Bureau; Jazz Pharmaceuticals: Honoraria, Research Funding, Speakers Bureau; Forma: Research Funding; Sun Pharma: Research Funding; Amphivena: Research Funding; Roche: Research Funding; AbbVie: Speakers Bureau; Alexion: Speakers Bureau; Onconova: Research Funding. Flower:Lentigen Technology Inc/Miltenyi Biotec: Research Funding. Cairo:Miltenyi: Research Funding; Technology Inc/Miltenyi Biotec: Research Funding; Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Nektar Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal